Saturated Fats: The Fat They Were Wrong About
Debunking the stigmatization of saturated fatty acids.

What we cover
For decades, saturated fats have been unfairly demonized because of claims linking them to heart disease and high LDL cholesterol. We break down why this oversimplification is misleading and how minimal evidence directly connects SFAs to chronic disease.
We revisit early studies and the Seven Countries Study, revealing how selection bias, inadequate data, and misinterpretations have contributed to a skewed view of saturated fats.
We expose the economic and industrial influences behind the fat narrative—highlighting how marketing campaigns and corporate funding have helped shape public guidelines against SFAs.
We clarify that LDL cholesterol isn’t inherently dangerous. It’s the oxidation of LDL, driven by unstable polyunsaturated fats, that creates health risks—a process often mistakenly attributed to saturated fats.
We review research suggesting that a higher intake of saturated fats may actually lower stroke risk, support better metabolic function, and even boost cognitive performance through benefits from medium-chain triglycerides (MCTs).
We also discuss how high-heat cooking methods, rather than the saturated fats themselves, are responsible for forming harmful compounds in meat, calling for a reassessment of our cooking practices.
Introduction
For decades, saturated fats have been stigmatized, largely due to claims surrounding saturated fats and their association with heart disease,[1] and the link between saturated fats and LDL cholesterol. While LDL cholesterol is often oversimplified to be known as “bad” cholesterol, reality is more nuanced. This oversimplification has perpetuated the myth that saturated fats are inherently unhealthy, with organizations like the American Heart Association grouping them with trans fats as “bad” fats to avoid. However, the widespread demonization of saturated fats lacks robust scientific backing and appears to be driven more by agenda than evidence. In reality, minimal substantial evidence directly links saturated fats to chronic diseases. Conversely, a higher intake of saturated fats (SFAs) may be more favorable to health than polyunsaturated fats (PUFAs). As recent research continues to challenge outdated beliefs, it’s becoming clear that saturated fats deserve a fair reassessment. This article explores the misconceptions surrounding saturated fats, examines the emerging evidence of their health benefits, and advocates for a more balanced approach to dietary guidelines.
Lipid Legends and Myths
To argue that saturated fats are beneficial for health, it’s essential to address and disprove the studies that claim otherwise. The scientific literature regarding dietary fatty acids is vast, but many early studies contain significant shortcomings. Unfortunately, the government recommendations to limit saturated fat intake are based upon these flawed studies.
Early Research
The foundation of this scientific literature can be traced back to 1930 when George and Mildred Burr, a husband-and-wife team, helped define what the scientific community now refers to as “Essential Fatty Acids” (EFAs).[2] Their series of two studies originally consisted of rats fed a completely fat-free diet, with all the known vitamins of the time being supplemented to their diet. In this original study, rats developed skin lesions, blood in urine, hair loss, and other negative health outcomes. However, in diets supplied with lard as 2% of total food consumption, superior growth was observed compared to the fat-free group and scaly skin was not present.[3] In the Burrs’ next study, it was shown that more unsaturated fats were better at eliminating these skin lesions in smaller amounts.[4] As a result, this is why linoleic acid has long been considered an “essential” fatty acid.
While this 94-year-old study is good for determining that fats are indeed a necessary part of these organisms’ diets, it does not paint the whole picture when it comes to the essentiality of unsaturated fats. Analytical methods for fats were far less sophisticated than they are today, and certain vitamins were not included in the diets due to them not being discovered at the time. As an example, vitamins B6 and B5 were not discovered or synthesized (respectively) until several years after this study was performed.[5] Furthermore, a subsequent study found that both vitamins B6 and B5 together permanently healed skin lesions and promoted normal growth that was presumably adversely affected by a low-fat diet alone.[6] Also take the following quote from the study into consideration:
“Every rat which received 5 milligrams of linoleic acid, either by the prophylactic, Curve I, or by the curative procedure, Curve II, eventually died with severe dermatitis. Two rats which received linoleic acid as a curative agent healed temporarily, but both of them had a recurrence before death.” [6]
These findings call for further research into the essentiality of unsaturated and saturated fats in both rats and humans, the latter being impossible to determine with research discussed so far. It is possible that the skin lesions and growth weight could have been eliminated by another factor or only temporarily cured in the original study. Given the imperfections in early analyses, more comprehensive studies are needed.
The Seven Countries Study
Continuing chronologically, the Seven Countries Study conducted by Ancel Keys supported his “diet-heart hypothesis” that is now the cornerstone on which the American Heart Association has proposed their advice to limit saturated fats. Keys’ study consisted of 12,763 people—only men—in seven different countries. However, the nutritional data for less than 100 people per country, about 500 men, were used.[7] This study concluded a strong correlation between saturated fat consumption and heart disease, leading to overall mortality. However, there are numerous flaws with the validity of this study:
- Selection Bias: Keys did not choose countries at random and could have easily picked these seven in an attempt to obtain stronger evidence for his pre-existing hypothesis. It is possible that he did not choose countries known to be paradoxical to this hypothesis, with popular ones being the Israeli Paradox and the French Paradox.
- Inadequate Data: Of the 12,763 men of the seven countries, only about 500 individuals’ dietary data was recorded in this study.[7]
- Cretan Fasting: According to a letter from the researchers in Public Health Nutrition, 60% of the Cretans that were being studied in the 1960s were fasting in 40 days of Lent, which means they were following dietary restrictions such as “periodic abstention from meat, fish, dairy products, eggs and cheese, as well as abstention from olive oil consumption on certain Wednesdays and Fridays”.[8] Evidently, this was not addressed anywhere in Keys’ reports. This means that the health of the Cretans cannot be attributed to any one factor in their diet during this period of time, whether it be from the restrictions, the lack of restrictions on olive oil aside from specific days, or the fasting itself.
It is important to note that this study was not a clinical trial, and therefore could not directly prove that saturated fat was the cause of coronary mortality.[9] Wrapping all these pieces into one suggests that perhaps the Seven Countries Study is not as supportive of its hypothesis as many organizations pin it as. In fact, more recent studies and meta-analyses have not supported this hypothesis.
A notable example is a 2016 study that re-examined unpublished documents and raw data from the Minnesota Coronary Experiment. The study found that while replacing saturated fat (SFA) with linoleic acid (LA), a type of polyunsaturated fat (PUFA), did lead to lower serum cholesterol levels, as Keys had hypothesized, but it did not correlate with an increased mortality rate. This challenges the idea that higher serum cholesterol—and by extension, SFAs—are inherently dangerous. In fact, there was a 22% higher risk of death for each 30 mg/dL reduction in serum cholesterol according to models analyzing the data.[10]
Now the question to consider is: why do these companies and organizations villainize saturated fat to this point despite the evidence against it being so weak?
Economic, Industrial, and Societal Influence – The Great Fat Conspiracy
In 1911, Procter & Gamble (P&G) created Crisco by hydrogenating cottonseed oil, a cheap byproduct of cotton farming, at a time when lard was the predominant cooking fat. Crisco aimed to replace lard at a significantly cheaper price. In an attempt to convince home cooks to switch from lard, P&G devised one of the largest advertising campaigns ever, with Crisco-fried food being distributed in the streets, free copies of Crisco-based recipes being given to women who bought Crisco, and boasting unverified health claims that hydrogenated cottonseed oil is superior for health and digestion than animal fats like lard.[11] However, partially-hydrogenated cottonseed oil produces trans fats, which are now known to be correlated with coronary heart disease. Specifically, a 2% increase in calories from trans fats was associated with a 23% increase in the risk for developing coronary heart disease.[12] Until this became known, the aggressive marketing campaign for Crisco continued.
The American Heart Association (AHA), from 1961 to today, has stated that SFAs are a primary factor in heart disease, issuing out advisories to limit saturated fats. In fact, this stance was influenced by Keys himself in 1957, who, with little evidence aside from his single study, convinced other AHA members to release this statement.[13] In this statement, they claimed that limiting SFAs and replacing them with PUFA-high vegetable oils would lower the risk of heart disease.
Allegedly, in 1948, the AHA received $1.4 million (nearly $19 million today) from Procter & Gamble, the company that had pioneered its way into the culinary world via Crisco, the cottonseed oil-based lard substitute high in PUFA compared to animal fats.[9,11] This substantial donation allowed the AHA to grow significantly and may have influenced their later claims. Since then, the AHA has continued to receive donations from various corporations, including pharmaceutical companies.[14]
By the time that data emerged suggesting that saturated fatty acids were not harmful to health, the claim that saturated fats increased heart disease risk had already become mainstream. This put pressure on researchers whose data did not support the prevailing paradigm. For example, a researcher named Ronald Krauss published papers in 2010 concluding that the paradigm regarding saturated fat required re-evaluation.[15,16] However, Krauss faced resistance in publishing these papers, and Keys’ colleague even wrote another paper refuting them.[9]
Today, the recommendation to limit saturated fat intake remains, with SFAs and trans fats lumped together as "bad" fats, while polyunsaturated fats (PUFAs) are labeled as "good" without any consumption limits. Misconceptions regarding cholesterol have also clouded most discussions about the health impacts of SFAs. There have been numerous clinical trials and studies supporting that this hypothesis should be re-evaluated. Here are some notable examples:
- Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease: Published in The American Journal of Clinical Nutrition in 2010, this study concluded that “Intake of saturated fat was not associated with an increased risk of CHD, stroke, or CVD,” and “Consideration of age, sex, and study quality did not change the results”.[16]
- Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73): Published in The BMJ in 2016, this analysis concluded that while serum cholesterol was lowered by replacing SFA with PUFA, there was a 22% higher risk of mortality for each 30mg/dL decrease in serum cholesterol.[10]
- The effect of replacing saturated fat with mostly n-6 polyunsaturated fat on coronary heart disease: a meta-analysis of randomised controlled trials: Published in Nutrition Journal in 2017, this study concluded that, when the trials that were “adequately controlled”, replacing SFA with omega-6 PUFA found no difference in major or total CHD events, or total/CHD mortality.[17]
This third paper, written by Steven Hamley, gets more interesting, as it digs deeper. The trials being analyzed had a control group (high SFA) and an experimental group (high PUFA). A glaring difference in these adequately controlled trials versus the inadequately controlled ones was the trans fatty acid (TFA) intake. TFAs, as described previously, are known for causing heart disease and various other problems in the human body.[12] They are artificial fats that are created from partially hydrogenating oils, creating double bonds that should not be in the fatty acid chain.
Given that margarines and shortenings contain a high omega-6 content, one would be led to believe they would be one primary food to replace SFAs in the experimental groups’ diet. It’s notable that in 11 trials discussed on this topic, all of them, whether indirectly or directly, provided the high SFA control group with more TFA than the other group.[17] Essentially, this means that the high SFA group ate more of the fats (trans fatty acids) that are known to cause the very problems attributed to saturated fats instead. When the trials are inadequately controlled, which they often are, SFA can easily be pinned due to this dogma. Below is a graphical representation of the controlled versus uncontrolled trials in major CHD events, total CHD events, CHD mortality, and total mortality:

These reduction numbers, also including results from the inadequately controlled trials, show that reductions were not significant. This suggests that much of the data blaming SFAs are misinterpreted or not properly controlled.
Conflation of trans fatty acids in trials, combined with the fact that SFA heightens LDL-Cholesterol (“bad” cholesterol) have been paramount to this false accusatory claim that SFAs are particularly unhealthy for the human cardiovascular system. Although an entire article could be written about this topic, below is a brief section outlining the primary reason why LDL-Cholesterol alone is not the problem.
Why LDL-Cholesterol Isn’t A Concern (in isolation)
To explain why LDL cholesterol isn’t a concern, first, some key points must be made clear. Cholesterol is the building block for cell structure in the human body, a precursor for a type of hormones, and is converted into vitamin D when UV rays penetrate the human skin.[18,19] The hormones that cholesterol are precursors to are called “steroid hormones”, and examples include cortisol, aldosterone, estrogen/testosterone, and progesterone. Steroid hormones are crucial for various functions of the human body such as reproduction and sexual characteristics (estrogen/testosterone), stress response (cortisol), and salt balance in the blood (aldosterone).[18] Vitamin D, also synthesized from cholesterol, is a key factor in bone health, muscle health, immune function, and even potentially preventing diabetes.[19]
Despite its importance, cholesterol is also often villainized, with food advertisements and labels claiming that products "lower cholesterol" and that generally lower cholesterol is healthier. High LDL cholesterol ("bad" cholesterol) is often blamed as the main problem, while HDL cholesterol is considered "good" cholesterol.
- LDL (Low-density lipoprotein) transports cholesterol from the liver for use in the general functions of cholesterol, like hormone production in the pituitary gland and cell membrane structure.
- HDL (High-density lipoprotein) transports excess cholesterol back to the liver for recycling/excretion.
LDL cholesterol itself, coined “bad” cholesterol, is not inherently bad. The main concern is oxidized cholesterol, which is what builds up on the artery walls, not unoxidized cholesterol. Excess oxidized cholesterol can lead to atherosclerosis, and thus high blood pressure, increasing the risk for heart attack and stroke.[20,21] Saturated fats are known to increase LDL cholesterol, so it’s assumed that higher LDL means higher chance for oxidized LDL and thus more health complications. However, the primary mechanism by which LDL is oxidized is often overlooked in this thought process.
LDL, the lipoprotein that carries (and is attached to) LDL cholesterol through the body, is oxidized and changed by free radicals and their byproducts. Free radicals are products that attack the double-bonds in polyunsaturated fats, causing oxidative stress in the body.[22,23] To learn more about this process and to understand it better, click here. This process essentially creates “aldehyde products”, [24] which then break down and modify the LDL lipoprotein, therefore modifying the entire LDL cholesterol molecule, and finally causing the LDL cholesterol molecule to stick to the walls of the arteries, causing the plaque buildup. This issue is often wrongly attributed to saturated fats but is actually caused by the unstable nature of PUFAs. In fact, saturated fats are far less susceptible to this process known as ‘lipid peroxidation’, and only PUFAs are particularly prone to it.[23]
Therefore, consuming more PUFAs and fewer saturated fats (SFAs) leads to increased oxidation of LDL cholesterol. PUFA oxidation is the primary starting point by which LDL cholesterol can turn into a substance harmful for human health.[25] To protect against this lipid peroxidation, antioxidants such as vitamin E can be consumed. This prevents the modification of LDL completely.[25]
In this context, ensuring proper body function means consuming more SFAs and limiting PUFAs. This is a perfectly reasonable hypothesis when confronted with this information. While some PUFAs are necessary for numerous bodily functions, their excessive consumption can have damaging effects.[23]
With evidence supporting that saturated fats are not harmful, the next step is to list the benefits of saturated fats and explain why they are healthy for the human body.
Proven Health Benefits of Saturated Fats
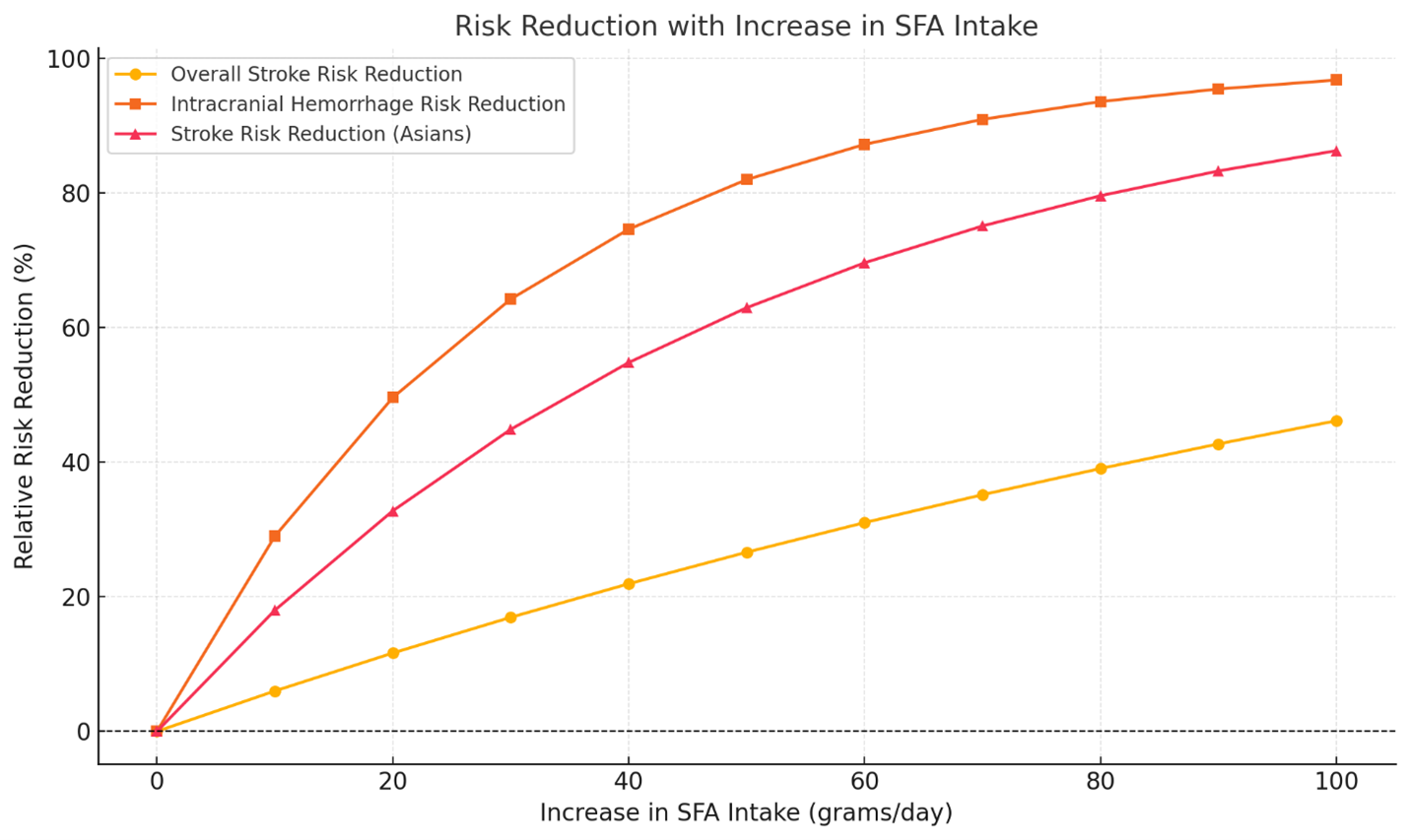
While saturated fats have been vilified for decades, there are clinically-supported benefits of consuming saturated fats. For instance, a 2019 meta-analysis published in NMCD found that a higher saturated fat intake was associated with a lower risk of stroke. Specifically, a 10g/day increase in SFA intake was associated with a 6% relative stroke risk reduction.[26] Clogged arteries, or atherosclerosis—which saturated fats are primarily blamed for causing—is a top risk factor for strokes.[27] If an increase in dietary saturated fat supposedly causes this buildup and inflammation, how could it possibly decrease risk of stroke? This evidence suggests that modern dietary guidelines should be reassessed.
A 2014 publication in Open Heart outlined similar risks associated with replacing SFA with PUFA that this article and Truthition’s other article has proposed, citing increased oxidization of LDL cholesterol, increased risk of cancer (see PUFA part 3), and increased risk of other cardiovascular events.[28] This article also called for dietary guidelines to “strongly reconsider” recommendations to limit saturated fat intake and replacing them with omega-6 PUFAs or carbohydrates.
Metabolic Effects
- Thyroid Function and Metabolism: The relationship between serum lipids and thyroid function is well-established. While some research indicates that polyunsaturated fats may decrease metabolic function and contribute to thyroid autoimmunity,[29] the effects of saturated fats are mixed. A recent study suggested that SFAs might modulate thyroid function, potentially decreasing it.[30] However, analyzing the methods of this study reveals that it did not account for other factors such as PUFA levels and other dietary and lifestyle influences. This study only provided correlations to blood samples and thyroid markers in the blood, and did not account for these other factors.
- Food Quality Matters: It is crucial to distinguish results between unhealthy high-saturated fat foods (e.g., heavily processed restaurant items) and healthy, whole foods. That is precisely what one study did, distinguishing different food groups and markers of thyroid function. This 2021 study concluded that whole foods with a high SFA content “not limited in consumption” showed positive effects on thyroid function.[31] Interestingly, high-glycemic index foods, like fruit juices, correlated positively with markers of increased thyroid function. Plant oils showed a weaker negative correlation, suggesting that they may decrease thyroid function.
Medium-Chain Triglycerides (MCTs):
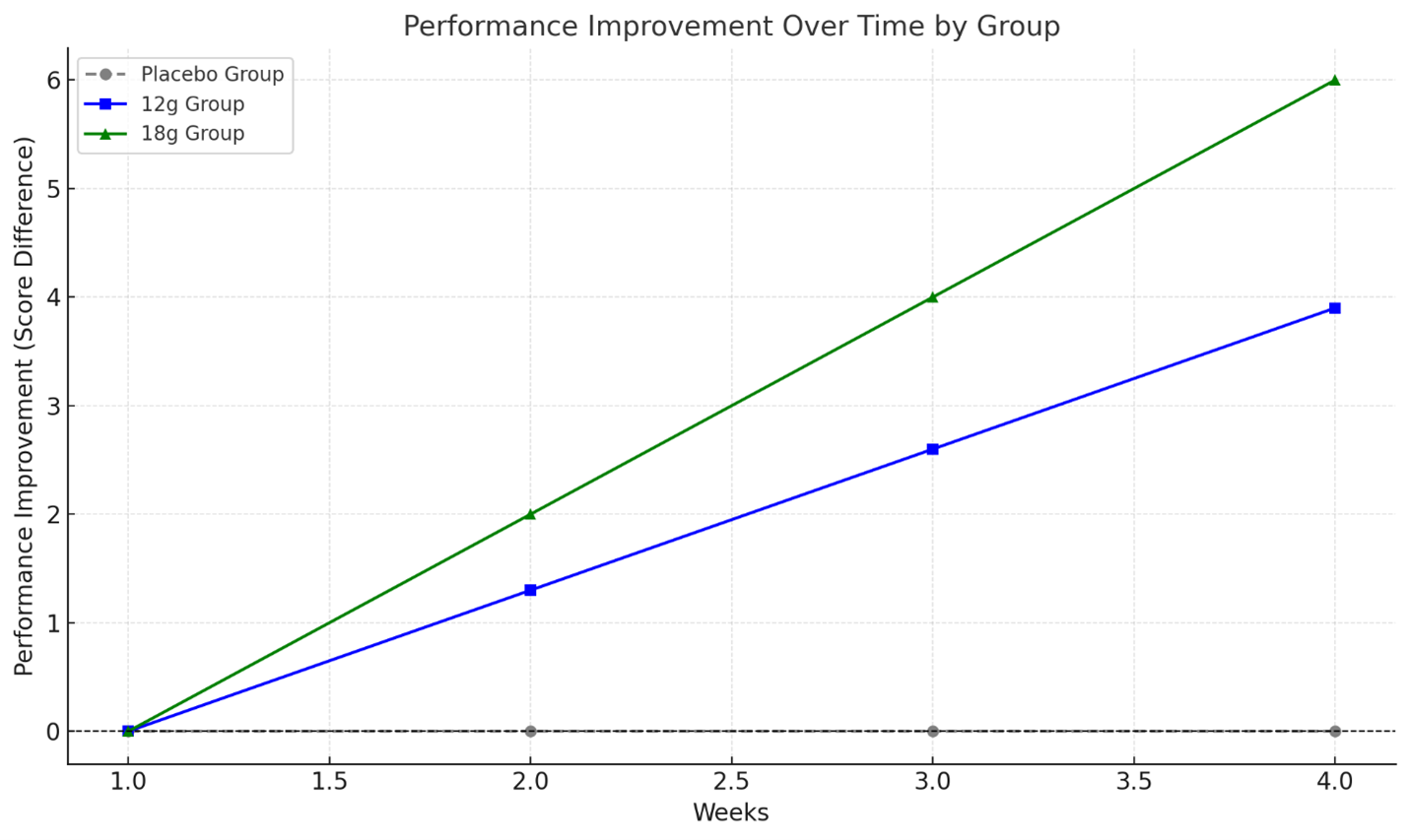
When looking at specific SFAs, there is a category called medium-chain triglycerides (MCTs). MCTs are medium-length fatty acid chain saturated fats, with notable sources being coconut oil, palm kernel oil, and dairy products. A 2020 controlled trial on healthy young adults concluded that supplementing 12+g / day of MCTs boosted cognitive function in tests.[32] There are other studies that support this as well: one trial on 20 Alzheimer’s Disorder (AD) patients suggested that long-term MCT supplementation may improve effects on working memory, short-term memory, and processing speed in those with mild to moderate AD.[33]
Stability of SFAs:
Unlike PUFAs, which are prone to oxidation, SFAs are far more resistant and stable within the body. Lipid peroxidation can cause various health issues (referenced in PUFA 3). Therefore, logically, replacing polyunsaturated fats with saturated fats in the diet could provide protection against the problems associated with rapid oxidation.
Cooking Methods of Saturated-Fatty Meat
Many studies villainize SFA because of their association with red meat, and red meat’s association with cancer. Red meat is often associated with saturated fats and therefore used in trials to assess the effects of their intake, such as in the food-group thyroid study mentioned earlier. However, the problem lies not with the SFAs but with high-heat cooking methods. When muscle meats (fish, chicken, beef, or pork) are cooked at over 300 degrees Fahrenheit, they create compounds called heterocyclic amines (HCAs) and polycyclic aromatic hydrocarbons (PAHs).[34] These compounds are not related to saturated fatty acids but to the cooking process itself. PAHs stick to the meat when it is exposed to smoke, and HCAs are formed when amino acids in the meat react to these high temperatures. These compounds have been known to be potentially carcinogenic and cause other problems in studies and trials alike, although PAHs are notably difficult to study.[35,36]
To avoid these compounds, meat can be cooked by reducing the amount of smoke it is exposed to from fat drippings, or by covering/marinating the meat in antioxidant-rich substances such as wine and herbs like oregano, thyme, basil, and rosemary. Additionally, the meat can be cooked in the oven beforehand to lessen the amount of time it is on the grill or in the pan.[37] It's also advisable to avoid processed meats like bacon, sausages, and hot dogs, which contain other carcinogenic compounds. Different cooking methods have not shown a decrease in these compounds, but HCAs are more likely to be carcinogenic than these compounds anyway.[38]
Given that cooking methods of these meats are associated with cancer and other issues, it supports the notion that saturated fatty acids may have been misunderstood and their effects misrepresented in many human trials. This contributes to the oversimplified narrative that saturated fat intake causes health problems, as these distinctions have commonly been ignored.
Conclusion
Saturated fatty acids (SFAs), found in fatty dairy, meats, oils, and other foods, have been unjustly demonized throughout history based on flawed research, biases, and possibly corporate agendas. Evidence suggests that consuming more SFAs may actually be more beneficial for human health compared to excessive intake of polyunsaturated fatty acids (PUFAs). Many studies claiming that SFAs pose health risks fail to account for critical nuances and rely on oversimplified data. These shortcomings include overlooking the mechanisms of LDL cholesterol oxidation, the impact of cooking methods on the formation of carcinogenic compounds, and conflating trans fats with saturated fats.
Specific SFAs, as discussed in this article, have been associated with lower risk of stroke, reduced lipid oxidation compared to PUFAs, potentially enhanced metabolism, and cognitive benefits. Given their significant role in human diets throughout history, SFAs warrant more impartial research to fully understand their effects—both positive and negative—on the body. It’s time to challenge the conventional dietary narrative that saturated fats should be minimized and replaced with PUFAs, and instead reassess SFAs with a balanced perspective rooted in modern science.
Citations
[1] "Saturated Fat." American Heart Association, 23 Aug. 2024, www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/saturated-fats.
[2] Mukhopadhyay, Rajendrani. "Discovering Essential Fatty Acids." ASBMB Today, 4 Oct. 2012, www.asbmb.org/asbmb-today/science/100412/the-discovery-of-essential-fatty-acids.
[3] Burr, George O., and Mildred M. Burr. "A New Deficiency Disease Produced by the Rigid Exclusion of Fat from the Diet." Journal of Biological Chemistry, vol. 82, 11 Feb. 1929, www.jbc.org/article/S0021-9258(20)78281-5/pdf.
[4] Burr, George O., and Mildred M. Burr. "Of the Nature and Role of the Fatty Acids Essential in Nutrition." Journal of Biological Chemistry, vol. 86, 9 Jan. 1930, www.jbc.org/article/S0021-9258(20)78929-5/pdf.
[5] Lindblom, Keith. "Celebrating the History of B Vitamin Research With ACS." ACS Axial, 2 Dec. 2016, axial.acs.org/cross-disciplinary-concepts/history-b-vitamin-research.
[6] Richardson, L. R., A. G. Hogan, and K. F. Itschner. "Vitamin B6, Pantothenic Acid, and Unsaturated Fatty Acids as They Affect Dermatitis in Rats." Journal of Nutrition, vol. 87, Sept. 1941, core.ac.uk/download/pdf/62789951.pdf.
[7] Astrup, Arne, et al. "Dietary Saturated Fats and Health: Are the U.S. Guidelines Evidence-Based?" Nutrients, vol. 13, no. 10, 22 Sept. 2021, www.mdpi.com/2072-6643/13/10/3305.
[8] Sarri, K., & Kafatos, A. (2005). The Seven Countries Study in Crete: olive oil, Mediterranean diet or fasting? Public Health Nutrition, 8(06). doi:10.1079/phn2005765
[9] Teicholz, Nina. “A short history of saturated fat: the making and unmaking of a scientific consensus.” Current opinion in endocrinology, diabetes, and obesity vol. 30,1 (2023): 65-71. doi:10.1097/MED.0000000000000791
[10] Ramsden C E, Zamora D, Majchrzak-Hong S, Faurot K R, Broste S K, Frantz R P et al. Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73) BMJ 2016; 353 :i1246 doi:10.1136/bmj.i1246
[11] Ramsey, Drew, and Tyler Graham. "How Vegetable Oils Replaced Animal Fats in the American Diet." The Atlantic, 26 Apr. 2012, www.theatlantic.com/health/archive/2012/04/how-vegetable-oils-replaced-animal-fats-in-the-american-diet/256155/.
[12] Clarke, Robert, and Sarah Lewington. “Trans fatty acids and coronary heart disease.” BMJ (Clinical research ed.) vol. 333,7561 (2006): 214. doi:10.1136/bmj.333.7561.214.
[13] Elkind, Mitchell S. V., et al. "The American Heart Association at 100: A Century of Scientific Progress and the Future of Cardiovascular Science: A Presidential Advisory From the American Heart Association." Circulation, vol. 149, no. 12, 2024, pp. e964–e985, doi:10.1161/CIR.0000000000001213.
[14] “Funding from Pharmaceutical and Biotech Companies and Device Manufacturers.” American Heart Association, 2021-2022, https://www.heart.org/-/media/Files/Finance/21_22_Pharma_Funding_Disclosure_0323.pdf.
[15] Siri-Tarino, Patty W et al. “Saturated fat, carbohydrate, and cardiovascular disease.” The American journal of clinical nutrition vol. 91,3 (2010): 502-9. doi:10.3945/ajcn.2008.26285.
[16] Siri-Tarino, Patty W et al. “Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease.” The American journal of clinical nutrition vol. 91,3 (2010): 535-46. doi:10.3945/ajcn.2009.27725.
[17] Hamley, S. The effect of replacing saturated fat with mostly n-6 polyunsaturated fat on coronary heart disease: a meta-analysis of randomised controlled trials. Nutr J 16, 30 (2017). https://doi.org/10.1186/s12937-017-0254-5.
[18] Hu, Jie et al. “Cellular cholesterol delivery, intracellular processing and utilization for biosynthesis of steroid hormones.” Nutrition & metabolism vol. 7 47. 1 Jun. 2010, doi:10.1186/1743-7075-7-47
[19] Shetty, Maya. "Vitamin D: Benefits, Sources, Deficiency." Stanford Lifestyle Medicine, 11 Mar. 2024, longevity.stanford.edu/lifestyle/2024/03/11/vitamin-d-benefits-sources-deficiency/.
[20] Moll, Jennifer. "What Is Oxidized Cholesterol?" Verywell Health, 15 Sept. 2022, www.verywellhealth.com/what-is-oxidized-ldl-698079.
[21] Truthition Team. "Under Pressure: The Truth About Blood Pressure." Truthition, Jan. 2025.
[22] Esterbauer, H et al. “Lipid peroxidation and its role in atherosclerosis.” British medical bulletin vol. 49,3 (1993): 566-76. doi:10.1093/oxfordjournals.bmb.a072631.
[23] Truthition Team. "Polyunsaturated Fatty Acids: The Real Killer III." Truthition, Jan. 2025.
[24] Pizzimenti, Stefania, et al. "Interaction of Aldehydes Derived from Lipid Peroxidation and Membrane Proteins." Frontiers in Physiology, vol. 4, 2013, www.frontiersin.org/journals/physiology/articles/10.3389/fphys.2013.00242.
[25] Epstein, F. H., Steinberg, D., Parthasarathy, S., Carew, T. E., Khoo, J. C., & Witztum, J. L. (1989). Beyond Cholesterol. New England Journal of Medicine, 320(14), 915–924. doi:10.1056/nejm198904063201407.
[26] Kang, Zhou-Qing et al. “Dietary saturated fat intake and risk of stroke: Systematic review and dose-response meta-analysis of prospective cohort studies.” Nutrition, metabolism, and cardiovascular diseases : NMCD vol. 30,2 (2020): 179-189. doi:10.1016/j.numecd.2019.09.028.
[27] "Atherosclerosis and Stroke." American Stroke Association, 8 Oct. 2023, www.stroke.org/en/about-stroke/stroke-risk-factors/atherosclerosis-and-stroke.
[28] James J DiNicolantonio - The cardiometabolic consequences of replacing saturated fats with carbohydrates or Ω-6 polyunsaturated fats: Do the dietary guidelines have it wrong?: Open Heart 2014;1:e000032.
[29] Lulian Xu, Zhenzhen Liu, Xu Xu, Qiwen Wan, Juanying Zhen, Li Jiang, Bernard Man Yung Cheung, Chao Li, Thyroid Autoimmunity is Associated with Dietary Fat Consumption, The Journal of Clinical Endocrinology & Metabolism, 2024;, dgae629, https://doi.org/10.1210/clinem/dgae629.
[30] Zhao, Wei, et al. "The Association Between Circulating Saturated Fatty Acids and Thyroid Function: Results From the NHANES 2011–2012." Frontiers in Endocrinology, vol. 15, 2024, doi:10.3389/fendo.2024.1405758. Accessed at www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2024.1405758.
[31] Brdar, D., Gunjača, I., Pleić, N., Torlak, V., Knežević, P., Punda, A., … Zemunik, T. (2021). The effect of food groups and nutrients on thyroid hormone levels in healthy individuals. Nutrition, 91-92, 111394. doi:10.1016/j.nut.2021.111394.
[32] Ashton, Jake S., et al. "The Effects of Medium Chain Triglyceride (MCT) Supplementation Using a C8:C10 Ratio of 30:70 on Cognitive Performance in Healthy Young Adults." Physiology & Behavior, vol. 229, 2021, 113252, doi:10.1016/j.physbeh.2020.113252.
[33] Ota, M., Matsuo, J., Ishida, I., Takano, H., Yokoi, Y., Hori, H., … Kunugi, H. (2018). Effects of a medium-chain triglyceride-based ketogenic formula on cognitive function in patients with mild-to-moderate Alzheimer’s disease. Neuroscience Letters. doi:10.1016/j.neulet.2018.10.048.
[34] "Chemicals in Meat Cooked at High Temperatures and Cancer Risk." Cancer.gov, 11 July 2017, www.cancer.gov/about-cancer/causes-prevention/risk/diet/cooked-meats-fact-sheet.
[35] Nowell, S., Coles, B., Sinha, R., MacLeod, S., Luke Ratnasinghe, D., Stotts, C., … Lang, N. P. (2002). Analysis of total meat intake and exposure to individual heterocyclic amines in a case-control study of colorectal cancer: contribution of metabolic variation to risk. Mutation Research/Fundamental and Molecular Mechanisms of Mutagenesis, 506-507, 175–185. doi:10.1016/s0027-5107(02)00164-1.
[36] Moorthy, Bhagavatula et al. “Polycyclic aromatic hydrocarbons: from metabolism to lung cancer.” Toxicological sciences : an official journal of the Society of Toxicology vol. 145,1 (2015): 5-15. doi:10.1093/toxsci/kfv040.
[37] Gerszberg, Deborah. "How to Safely Grill: Decrease Your Risk for Cancer." Columbia Surgery, www.columbiasurgery.org/news/2015/08/05/how-safely-grill-decrease-your-risk-cancer. Accessed Jan. 2025.
[38] Wang, Jun et al. “Carcinogen metabolism genes, red meat and poultry intake, and colorectal cancer risk.” International journal of cancer vol. 130,8 (2012): 1898-907. doi:10.1002/ijc.26199.
Comments For 6
You must be logged in to comment.